
{kind=link}
One of the most pernicious myths promoted by antivaxxers during the pandemic is that vaccination against COVID-19 during pregnancy is dangerous. One only has to search an antivax activist site using the terms “pregnancy” and “COVID-19 vaccine” (as I did here for Children’s Health Defense and the Brownstone Institute as examples) to produce a long list of fear mongering articles about how supposedly vaccination during pregnancy increases the rate of fetal death and miscarriage, “attacks the placenta and ovaries,” along with various false and misleading claims of a “cover-up” of adverse outcomes in pregnancy associated with vaccination. Unsurprisingly, when longtime antivax activist Robert F. Kennedy Jr. took over as Secretary of Health and Human Services in February, it didn’t take long for him to put his finger on the scales to alter government policy so that the Centers for Disease Control and Prevention no longer recommends COVID vaccination for pregnant women and “healthy” children and announcing it on X, the hellsite formerly known as Twitter:
Of course, as regular readers of this blog would know, there is no evidence that COVID-19 vaccination is associated with any of those harms when administered during pregnancy, and lots of evidence that they are not. Indeed, it is the overwhelming scientific consensus that COVID-19 vaccines are safe and effective during pregnancy, with numerous studies demonstrating that they are safe for the developing fetus. Indeed, vaccination in general during pregnancy, not just with COVID vaccines, is safe for the mother-infant dyad. Indeed, a recently updated meta-analysis shows that COVID-19 vaccination during pregnancy reduces maternal SARS-CoV-2 infection risk by 48%, with mRNA vaccines showing higher efficacy (52% vs. 43% for inactivated), decreases maternal hospitalization risk by 42% and the risk of severe outcomes by 50%, while improving neonatal outcomes improved, including reduced infection, preterm birth, stillbirth, and neonatal death, as well as concluding that third-trimester vaccination likely offers better protection against preterm birth.
In contrast, you know what is dangerous to developing fetuses and pregnant individuals? It’s not what antivaxxers claim, obviously. I expect that you probably guessed it right away: SARS-CoV-2 infection, resulting in COVID-19 disease. Not only does it result in increased risk to the pregnant individual, including of pre-eclampsia, but to the fetus. For example, pregnancy is a risk factor for severe disease, a risk that remains elevated for up to a month after giving birth. Moreover, COVID-19 infection during pregnancy has been associated with increased risks of preterm birth, stillbirth, intrauterine growth restriction, requiring care in a neonatal intensive care unit (NICU), and adverse neurodevelopmental outcomes.
This brings us to today’s topic, a study published last week in Obstetrics & Gynecology by Shook et al and a research group from Harvard and Massachusetts General Hospital, entitled Neurodevelopmental Outcomes of 3-Year-Old Children Exposed to Maternal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Utero. Spoiler alert: It turns out that, in addition to all the bad things that COVID-19 infection has been shown to cause during pregnancy, COVID-19 infection during pregnancy is also associated with an increased risk of receiving a neurodevelopmental diagnosis, including autism, by age 3.
COVID-19 during pregnancy and neurodevelopmental outcomes
Before I discuss the study itself, it’s worth describing why investigators might suspect that SARS-CoV-2 infection during pregnancy might increase the risk of neurodevelopmental disorders in the infant. The authors tell it straight up right in the introduction:
A substantial body of evidence links maternal infection during pregnancy to adverse neurodevelopmental outcomes in offspring. Large national registry studies have reported increased risks of neuropsychiatric disease such as autism spectrum disorder, cognitive delay, schizophrenia, and mood disorders after in utero exposure to maternal infections. 1–4 For example, a Swedish study of 2.3 million births found a 30% increase in risk for autism spectrum disorder among the offspring of women hospitalized with an infection during pregnancy, 2 and a subsequent analysis of 1.8 million births identified a 79% increase in risk for autism spectrum disorder and a 24% increase in risk of major depression among offspring exposed to any maternal infection in pregnancy, whether hospitalized or not. 3 Relevant to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is only rarely vertically transmitted, 5 adverse offspring neurodevelopmental effects from maternal viral infection can occur even without vertical transmission, as has been observed with influenza. 6–8
The link between maternal infection and offspring neurodevelopmental disorders, even in the absence of vertical pathogen transmission to the fetus, has been demonstrated in animal models. Data from rodent and nonhuman primate models demonstrate that maternal immune activation disrupts normal fetal brain development through alterations in neuronal migration, synaptic function, and microglial activity. 9–16 We therefore hypothesized that, as with other viral and bacterial infections in pregnancy that are only rarely vertically transmitted, maternal SARS-CoV-2 infection could be associated with increased rates of neurodevelopmental diagnoses in offspring.
The authors then cite previous work by their group, for example, this 2023 study, that observed that “male but not female offspring born to mothers with a positive SARS-CoV-2 polymerase chain reaction test result during pregnancy were more likely to receive a neurodevelopmental diagnosis in the first 12 months after delivery, even after accounting for preterm delivery.” A contemporaneous NPR article describing the study noted that the abnormalities found in the group born after COVID-19 infection during pregnancy were of the type that often presaged a diagnosis of autism but, given that it was only 2023, the cohort was too young for any conclusions to be made. They also noted that “not all studies have identified this elevated risk, particularly those that did not consider clinical diagnoses or employed shorter-term follow-up.” As a result, they wanted to do this study now that they could examine neurodevelopmental outcomes out to 36 months after birth.
The cool thing about this study was that it was designed to look at live births during the early stages of the pandemic, so that only a very small percentage of the pregnant individuals studied actually received any COVID-19 vaccines. Let’s take a look. The investigators did a retrospective cohort study of 18,124 live births to individuals who delivered between March 1, 2020, and May 31, 2021, within the Massachusetts General Brigham health system. The exposure of interest was maternal SARS-CoV-2 infection, which was defined as a positive SARS-CoV-2 polymerase chain reaction test result during pregnancy, while the outcome of interest was any neurodevelopment diagnosis by the age of 36 months, defined and identified using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision diagnostic codes. The authors then looked to determine if there were any association between SARS-CoV-2 exposure during pregnancy and neurodevelopmental diagnoses using logistic regression models and controlling for confounders including maternal age, race and ethnicity, insurance type, hospital type, and preterm birth.
So what did the authors find? First of all, because this was early in the pandemic, only 8% of uninfected mothers had received at least one COVID-19 vaccine dose during pregnancy, compared with only 2% of mothers in the cohort who tested positive for SARS-CoV-2, with only 13 infections identified in women who had received at least one dose. Moreover, 65% of the infections observed occurred during the third trimester.
Of the 861 children whose mothers had COVID-19 while pregnant, 16.3% were diagnosed as having at least one neurodevelopmental condition by age 3, compared with 9.7% of the 17,263 children from COVID-negative pregnancies. After adjusting for maternal age, race, insurance and hospital type, and preterm birth, COVID-19 infection in pregnancy was linked to a 29% higher risk of a neurodevelopmental disorder in children.
Here’s the unadjusted data summarized in a table:
As you can see, the risk of any neurodevelopmental diagnosis by age three is significantly elevated in the cohort who had been exposed to SARS-CoV-2 during pregnancy. When the authors adjusted for various risk factors associated with neurodevelopmental diagnoses, the correlation still held:
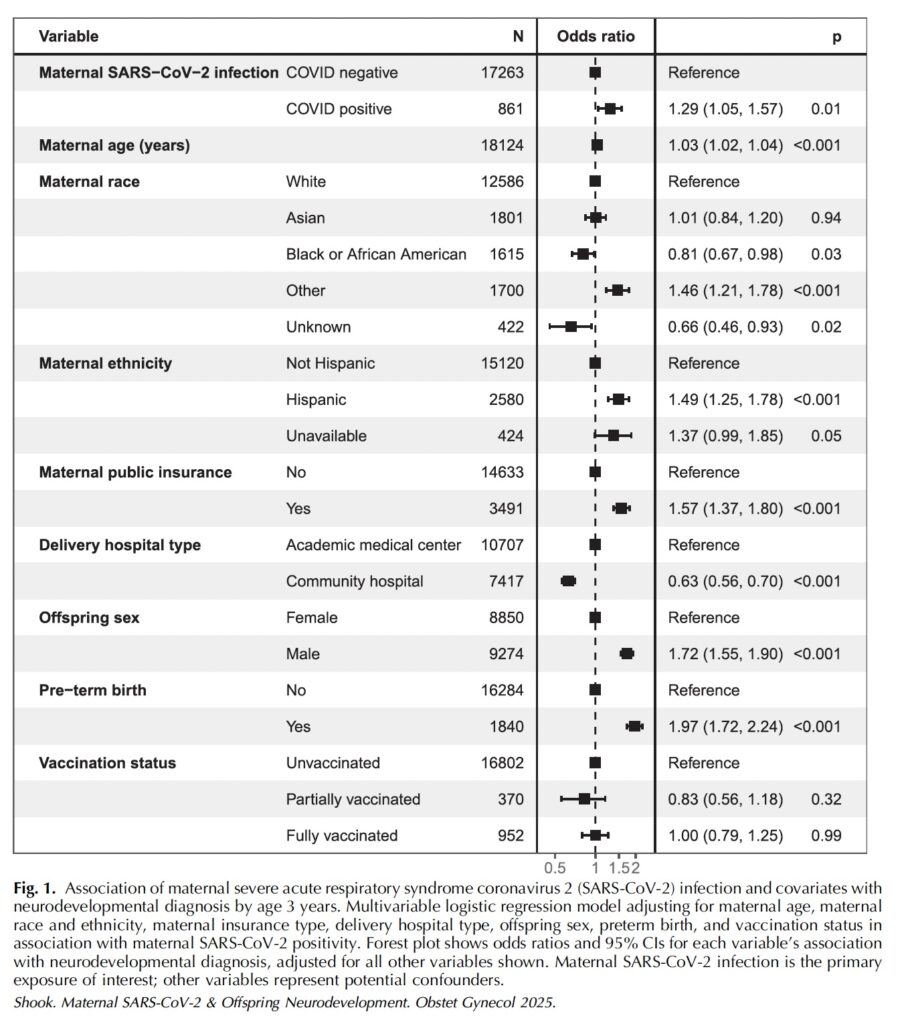
I will admit that an odds ratio of 1.29, portending a 29% increased risk of a condition, is not a huge increased risk in a study of this type, but it does so far appear to be real. Moreover, the risk appears to be highest if the COVID-19 exposure occurs during the third trimester:
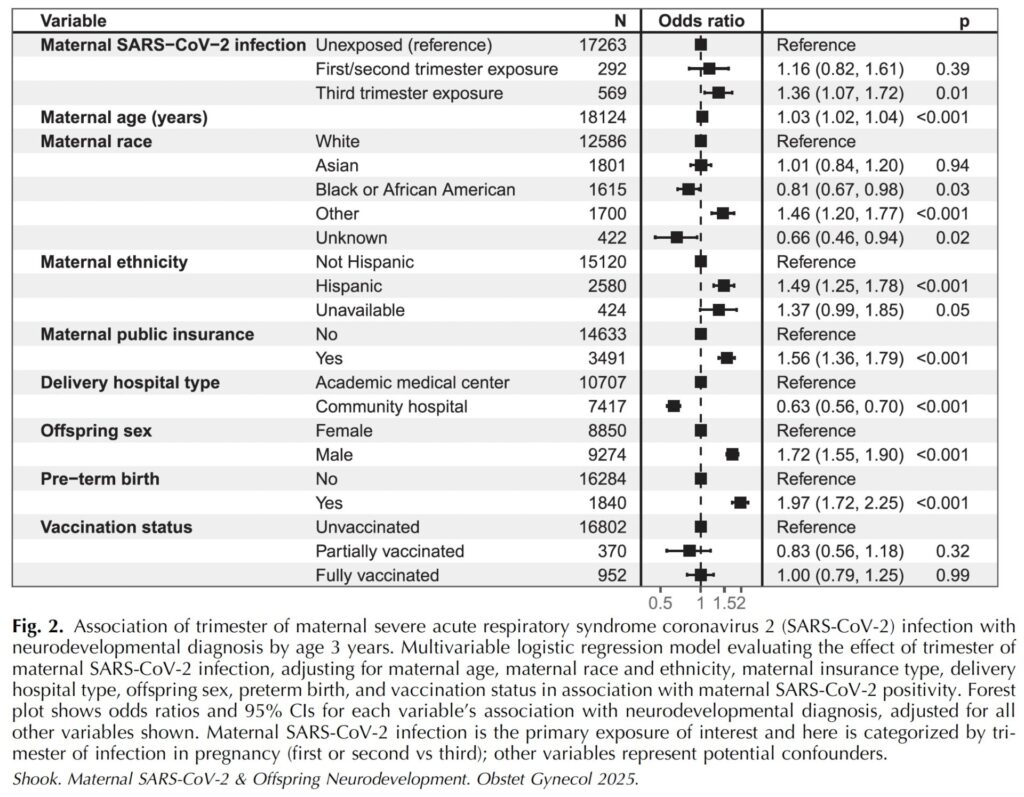
According to the analysis of this cohort, however, the group of infants at highest risk for a neurodevelopmental diagnosis are boys whose in utero exposure to SARS-CoV-2 occurred during the third trimester:
Among male offspring, third-trimester maternal SARS-CoV-2 infection was significantly associated with an increased risk of neurodevelopmental diagnosis at age 3 years (aOR of 1.43, 95% CI, 1.05–1.91, P5.02 (Fig. 3). The magnitude of risk in female offspring with third-trimester exposure was more modest and not statistically significant (aOR 1.27, 95% CI, 0.85–1.85, P5.23; Appendix 3, available online at http://links.lww.com/AOG/E396).
The authors note that these findings align with what was already known before about infections during fetal development as a potential trigger for neurodevelopmental disorders, noting that the “sex-specific vulnerability aligns with previous human and animal data indicating greater susceptibility of the male placenta and fetal brain to maternal immune activation, 11,27–29 including in the setting of SARS-CoV-2. 30–32” Looking up the references cited, I noted with interest that there is indeed a lot of evidence supporting a link between maternal immune activation and childhood neurodevelopmental disorders, including autism spectrum disorder, attention-deficit/hyperactivity disorder and Tourette syndrome and that there are animal studies that suggest that animal models suggest that there are different mechanisms for male and female fetuses in how maternal immune activation can impact neurological development, with males exhibiting more acute social and learning-related behavioral abnormalities and females exhibiting elevated anxiety-related behavior as adults. How well these findings in mice map to humans is unknown, but the authors did find distinct mechanisms in males and females, which led them to entitle their paper “Females are not just protected males.”
These observations are particularly notable in light of their biological plausibility. We have previously shown that SARS-CoV-2 exposure affects the transcriptional programs and biological function of human placental Hofbauer cells, 35 which may serve as a proxy cell type reflecting the effects of maternal exposures on fetal brain microglia, immune cells that play a key role in early neurodevelopment. 36 Maternal SARS-CoV-2 infection has been demonstrated to be associated with sex-specific patterns of immune activation in the placenta, 30 altered synaptic pruning behavior of induced microglialized placental cells, 35 and more deleterious effects on the male fetal brain in a humanized ACE2 knock-in mice. 32 Maternal SARS-CoV-2 infection also has been shown to be associated with activation of fetal–placental complement pathways, contributing to fetal inflammation independent of fetal virus exposure, 37 as well as compromised blood vessel integrity and disrupted microglial organization associated with cortical hemorrhages in the human fetal brain exposed to maternal SARS-CoV-2 infection. 38,39 Taken together, these studies provide a potential mechanism by which maternal SARS-CoV- 2 infection may contribute risk to the developing fetal brain even in the absence of vertical transmission.
You don’t have to understand all of the technical terms above to realize that what the authors are saying is that SARS-CoV-2 exposure and infection can affect the biology of the placenta and immune cells playing a key role in the development of the nervous system and that the effects of maternal immune activation seem to be more severe in male fetuses.
Of course, this study is hardly bulletproof and hardly the last word. For one thing, it’s retrospective, which means that there can always be confounders that might not have been accounted for. For another thing, as large as the cohort is, it’s still only a single institution, even if that institution includes Mass General Hospital and Harvard. The authors note that there was also a lack of a truly systemic diagnostic assessment, but further argued that, even if that were the case, it would tend to bias the results towards the null; i.e., make it more likely that any correlation between SARS-CoV-2 exposure and neurodevelopmental diagnoses by age 3 will be missed and to decrease the observed magnitude of any odds ratio calculated if a correlation is observed. They also admitted that, although there was universal screening for SARS-CoV-2 in the labor and delivery units during the period of time encompassing this cohort, it is nonetheless possible that asymptomatic COVID-19 could have been missed in some patients. However, like the lack of systematic diagnostic assessment in every case, they argue that this any misclassification of asymptomatic SARS-CoV-2 cases as negative would also tend to bias the findings of the study towards the null hypothesis.
As with all studies of this type, the key will be two-fold:
- What is observed in this cohort as time goes on, and I’m sure that the authors plan on re-analyzing their data every couple of years to document just that.
- Replication in other studies and cohorts. This will require other databases and other cohorts that include a large number of births early in the pandemic before vaccines were available, a necessary precondition to have a “cleaner” dataset.
The overall point, however, is that if you look at existing high-quality evidence about the safety and efficacy of COVID-19 vaccination during pregnancy, there are two strong conclusions. First, the vaccines are indeed safe and effective when administered during pregnancy. I realize that antivaxxers frequently invoke all the stuff that I discussed above regarding maternal immune activation interfering with neurodevelopment and potentially increasing the risk of autism and neurodevelopmental disorders, particularly in boys, but ask yourself this: What activates the immune system more, infection or vaccination? Then note that there is as yet no high-quality evidence suggesting that COVID-19 vaccination (or any vaccination, for that matter), increases the risk of autism or neurodevelopmental disorders, the recent “study” by the antivax McCullough Foundation being touted by antivaxxers right now notwithstanding. (I will have to address this “report” at some point, but it’s 82 pages long, and I just didn’t have time this weekend. Nor will I link to it now.) Next, this study and a number of other lines of evidence strongly suggest that it is actually SARS-CoV-2 infection, even just exposure, that is the real danger to developing fetuses, particularly in the third trimester. Granted, the risk still remains low, and the increased risk is low, but it appears to be real. If you add that increased risk of neurodevelopmental disorder due to COVID-19 to the known increased risk of stillbirth, intrauterine growth retardation, and the like, and there is an even stronger rationale for maternal immunization.
Indeed, if one looks holistically—yes, I used that word—at the existing scientific evidence, it suggests that infection in general during pregnancy is a risk factor for neurodevelopmental disorders. Perhaps the most studied example is congenital rubella syndrome, first described in 1971, in which infection with rubella during pregnancy produces a congenital syndrome, in addition to which there is a highly elevated risk of autism. While more recent evidence has cast some doubt on the strength of this correlation, it is generally accepted that fever during pregnancy is associated with an elevated risk of neurodevelopmental disorders like autism, and the most common cause of fever is infection.
Not that any of this science or these facts stops antivaxxers. For example:
Here’s the funny thing, though. I’ve perused all the usual antivax sources, and I’ve seen almost no mention of this study. I find that telling. If the study had any obvious flaws that antivaxxers could point to, someone at Children’s Health Defense, the Brownstone Institute, or any of a number of antivax blogs, Substacks, and websites would have written a detailed takedown by now, given that the study was published on October 30. Three or four days is plenty of time for this, as anyone who’s been following the disinformation space would know.
The bottom line is that the myth that vaccination during pregnancy, be it with mRNA-based COVID vaccines or vaccines that have long been on the CDC recommended schedule, harms the developing fetus and/or causes neurodevelopmental conditions like autism is a pernicious one. Unfortunately, now that we have a rabid antivaxxer in charge of public health and vaccine policy, both infants and their mothers will suffer unnecessary harm from policies not based in science and evidence. Such is the world that we are living in now.